The University of Bristol Sponsors Biomarker Internship at SSL
Biomarkers are an important tool to help reduce rejection
Wouldn’t it be wonderful if doctors could treat patients as individuals, taking into account their genes, environment and lifestyle, rather than imposing a one-size-fits-all approach?
This is referred to as precision medicine and is a rapidly growing field. In the field of heart transplants, precision medicine is important because it can improve patient care, post-transplant health, and post-transplant longevity.
Therefore, Santorini Scientific have lead an internship, funded by the University of Bristol, to explore the role of biomarkers of cardiac rejection in the field of precision medicine.
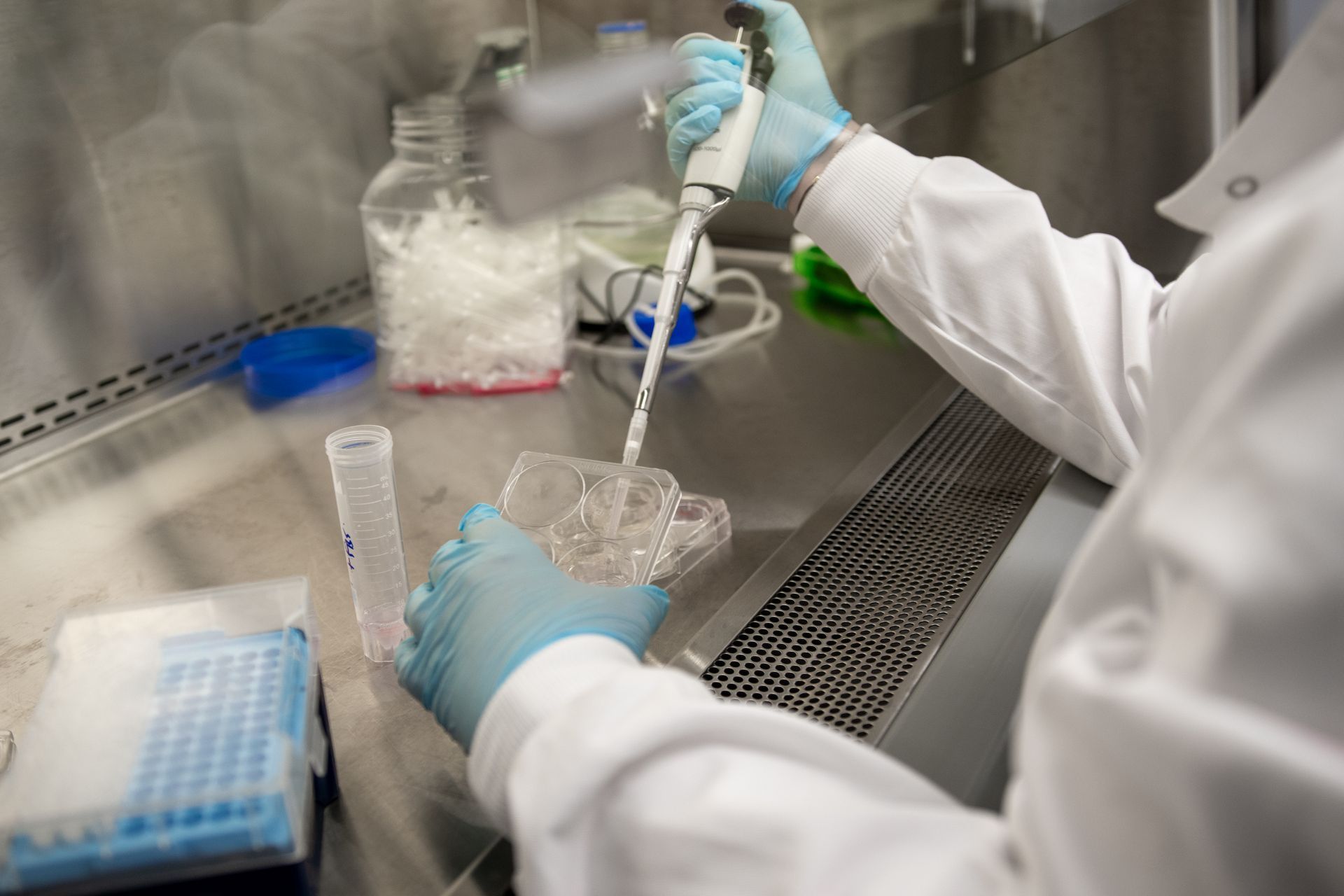
Biomarkers (shorthand for “biological marker”) are naturally occurring medical signs which can be used to identify how well someone’s body responds to a treatment for a disease or condition. They are typically used as a tool for diagnosis and to evaluate clinical pathways.
They are usually split into two main types: exposure and disease, and four main characteristics: molecular, histologic, radiographic and physiologic.
Gene expression profiling (GEP) is a type of genomic biomarker can be used to profile peripheral blood mononuclear cells (PBMC) and, as a recent research paper highlights “identify 11 differentially expressed genes and help with detection of moderate and severe acute cellular rejection in stable heart transplant recipients”.
The researchers add, “In recent years, the utilization of GEP of PBMC for identifying differentially expressed genes to diagnose acute antibody-mediated rejection and cardiac allograft vasculopathy has yielded promising results” [Khachatoorian, Khachadourian et al., 2021].
Further research published this year (2021) investigates “recent advances in the field of non-invasive biomarkers to detect allograft rejection after heart transplant”. Biomarkers could be used to measure level of rejection without requiring an invasive endomyocardial biopsy (EMB) which is the current preferred method for cardio allograft monitoring.
The researchers note that “Heart transplantation is the standard of care for end-stage heart failure refractory to medical therapy. Although significant strides have been made in long-term survival, graft dysfunction caused by acute rejection remains a leading cause of morbidity and mortality.” [Qian, Shah and Agbor-Enoh, 2021]
Primary graft dysfunction (PGD) rates vary from 20-40%, report researchers Ludhwani, Abraham and Kanmanthareddy in a 2021 article.
They note “Nearly half of heart transplant recipients developing rejection after 7 years of transplantation have evidence of antibody-mediated rejection. The overall prevalence of CAV [cardiac allograft vasculopathy] increases with time. CAV is the leading cause of death between 1 and 3 years after transplantation. CAV accounts for 17% of death after 3 years.”